Here are links to CLL information provided by the National Institute of Health, National Cancer Institute.
Professional Link - a more general information source including diagnosis, staging, etc.
Adult Treatment Editorial Board. PDQ Chronic Lymphocytic Leukemia Treatment. Bethesda, MD: National Cancer Institute. Available at: https://www.cancer.gov/types/leukemia/hp/cll-treatment-pdq. [PMID: 26389470]
Patient Link PDQ Adult Treatment Editorial Board. PDQ Chronic Lymphocytic Leukemia Treatment. Bethesda, MD: National Cancer Institute. Available at: https://www.cancer.gov/types/leukemia/patient/cll-treatment-pdq. [PMID: 26389485]
Diagnosis. Clusters of Differentiation (CD) - used to diagnose (differentiate) B cells. Normal from malignant, and differentiation within malignancies. Chronic lymphocytic leukemia/small lymphocytic lymphoma is differentiated by CD5, CD19, CD20, and CD23.
CLL cell trafficking. Chemokine gradients provide a "force" to encourage migration of CLL cells from bone marrow to lymph nodes (and vice versa) and lymph nodes to blood (and vice versa). Additionally, chemokines (CCL3, CCL4, and others) secreted by CLL cells may play a role in creating supportive microenvironments for CLL growth and proliferation in addition to chemokines secreted by stromal cells.
Glossary and Abbreviations
mAbs - monoclonal antibodies, they deplete B cell lineage or plasma cells by signaling disruption
Bcl-2 - B-cell lymphoma-2,
BCR - B Cell Receptor
BTK - Bruton Tyrosine Kinase,
BTKi - Bruton Tyrosine Kinase inhibitor
cBTKi - covalent (irreversible) BTKi
ncBTKi - noncovalent (reversible) BTKi
CARs - chimeric antigen receptors
CAR-T - chimeric antigen receptor-modified T cells
TAAs - Tumor Associated Antigens, examples include CD19, CD20, CD22, and CD38
Treatment Options and Algorithm
Six types of treatment are used:
Watchful waiting
Targeted therapy
Chemotherapy
Radiation therapy
Immunotherapy
Chemotherapy with bone marrow or peripheral blood stem cell transplant
"The treatment landscape for patients with chronic lymphocytic leukemia (CLL) has changed considerably with the introduction of very effective oral targeted therapies (such as Bruton tyrosine kinase inhibitors and venetoclax) and next-generation anti-CD20 monoclonal antibodies (such as obinutuzumab). These agents lead to improved outcomes in patients with CLL, even among those with high-risk features, such as del17p13 or TP53 mutation and unmutated immunoglobulin heavy chain (IGHV) genes. Selecting the right treatment for the right patient requires consideration of disease characteristics and prior treatment sequence, as well as patient preferences and comorbidities. The CLL-International Prognostic Index (CLL-IPI) remains the best-validated tool in predicting the time to first therapy among previously untreated patients, which guides selection for early intervention efforts. This review summarizes our current approach to the management of CLL, right from the time of diagnosis through relapsed disease."
Insight into the critical role of B-cell receptor signaling for the pathogenesis of chronic lymphocytic leukemia (CLL) led to the development of targeted therapies directed at key regulators of cell survival. Agents targeting B-cell lymphoma-2 protein (Bcl-2), Bruton's tyrosine kinase (BTK), and phosphatidylinositol 3-kinase (PI3K) are approved for treatment of CLL, and have significantly improved the disease management.
Bruton's tyrosine kinase (BTK) is a member of the TEC kinase family. Bruton's tyrosine kinase (abbreviated Btk or BTK), also known as tyrosine-protein kinase BTK, is a tyrosine kinase that is encoded by the BTK gene in humans. BTK plays a crucial role in B cell development. (See this Wikipedia link for more information.) A tyrosine kinase is an enzyme.
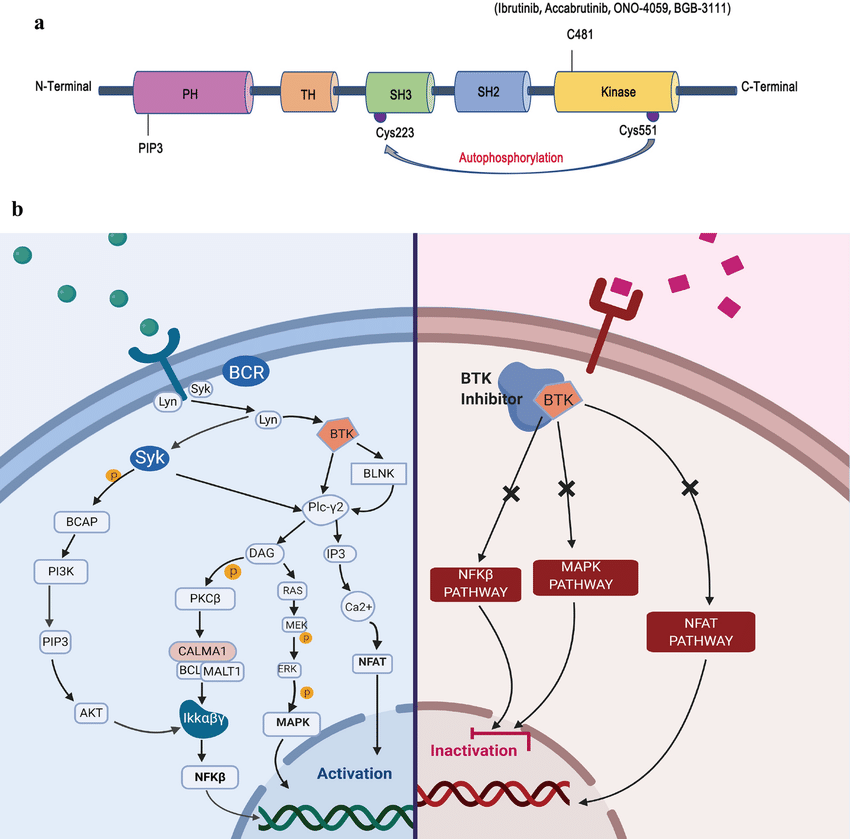
BTK is predominantly expressed in hematopoietic cells. In B lymphocytes, BTK is primarily required for B cell receptor (BCR). Upon BCR activation, BTK is recruited to the BCR signaling complex, where BTK activity is positively regulated by phosphorylation events. Activated BTK in turn phosphorylates PLC$\gamma$2 to induce downstream transcription factors such as NF-$\kappa$B, NF-AT and ERK1/2. In addition to BCR, BTK also participates in the signaling pathways of chemokine receptors in B cells, including CXCR4 and CXCR5. Therefore, BTK plays essential roles in regulating B cell development, survival, proliferation, differentiation, activation and chemotaxis.
Elevated expression and activity of BTK have been ubiquitously documented in many types of B cell malignancies. Aberrant BTK activities play crucial driving roles in the pathogenesis of B cell malignancies, including malignant B cell survival, proliferation and migration, and thus have been recognized as a prime therapeutic target for the treatment of B cell malignancies.
Signaling pathway disruptions by BTKi agents. Covalent (irreversible) Bruton's tyrosine kinase inhibitors (BTKi) bind to the C481 residue of BTK and blocks the ATP-binding pocket, thereby preventing catalytic activity.
BTK pathway disruption.
Resistance to covalent binding. Resistance to covalent BTK inhibitors is best understood in CLL, in which mutations at the BTK C481 amino acid residue impair drug binding and thereby restore the catalytic activity of BTK. In addition, activating mutations in phospholipase C gamma 2 (PLC$\gamma$2), a direct substrate of BTK, render malignant cells less reliant on BTK.
Hypermorphic mutation of phospholipase C, gamma 2 acquired in ibrutinib resistant CLL confers BTK independency upon BCR activation : "While the C481S mutation found in BTK has been shown to disable ibrutinib's capacity to irreversibly bind this primary target, the detailed mechanisms of mutations in PLCG2 have yet to be established. Herein we characterize the enhanced signaling competence, BTK independence, and surface immunoglobulin dependence of the PLCG2 mutation at R665W which has been documented in ibrutinib-resistant CLL. Our data demonstrate that this missense alteration elicits BTK-independent activation after B-cell receptor engagement, implying the formation of a novel BTK-bypass pathway. Consistent with previous results, PLCG2 R665W confers hypermorphic induction of downstream signaling events. Our studies reveal that proximal kinases SYK and LYN are critical for the activation of mutant PLCG2 and that therapeutics targeting SYK and LYN can combat molecular resistance in cell line models and primary CLL cells from ibrutinib-resistant patients. Altogether, our results engender a molecular understanding of the identified aberration at PLCG2 and explore its functional dependency on BTK, SYK, and LYN, suggesting alternative strategies to combat acquired ibrutinib resistance. and/or IAD35546 panel, pipeline version 1.2, amplicons in 2 pools, 48kb panel size, 98.9% coverage."
BCL-2 is a family of proteins that regulate cell death by controlling the cell death mediators BAX and BAK. When natural cell death is warranted, pro-apoptotic proteins bind to, and inactivate, BCL-2 to prevent it from stopping cell death. CLL cells over-express BCL-2 allowing for increased survival of the CLL cells. Chemical agents, such as Venetoclax are designed to phamacologically inhibit the pro-survival proteins such BCL-2.
"Venetoclax is the first BH3 mimetic drug and a selective BCL-2 inhibitor that has received FDA
approval. The main advantage of venetoclax over other agents is that it has a high binding
affinity for BCL-2 receptors and it very selectively inhibits BCL-2, maintaining anti-apoptotic
activity in cancer cells. Moreover, monotherapy with this agent facilitates a rapid reduction in
the disease burden with an overall good response rate. This drug has proved to provide good
therapeutic responses in CLL patients irrespective of the presence of adverse clinical or genetic
features, including in patients with relapsed or refractory forms of CLL. We believe that the
emergence of novel combination therapies, including venetoclax and immunotherapy,
will transform the treatment landscape for patients with relapsed CLL, particularly those with
(del 17p) CLL, which carries a very poor prognosis."
"Inhibitors of PI3Kδ hold great potential for the therapy of CLL and B cell malignancies. After
initially exciting efficacy results with idelalisib, the first in class inhibitor, the emergence of
unexpected and unpredictable autoimmune toxicities, worse in less heavily treated and younger
patients, has decreased the use of the currently available inhibitors. Newer drugs in development
are attempting to reduce toxicity with novel schedules and/or combinations. This article reviews
the clinical data on efficacy and toxicity across the class, and discusses ongoing efforts to
understand and mitigate the likely on-target autoimmune toxicity."
Splenic tyrosine kinase (SYK), a kind of tyrosine kinase which does not bind with a specific receptor, transmits signals from B-cells and has been considered an important adaptive immune receptor signal. SYK inhibitor therapy inhibits B-cell maturation and survival by inhibiting the signaling kinase SYK of B-cells. SYK is activated by (lg)E and lgG which are Fc receptors linked to immunoglobulins, the activation occurs in the microenvironment of some patients and causes weak phagocytic response. Therefore, SYK is critical in maturation and survival process of the entire lineage of B-cell. Thus, the inhibition for SYK has been considered as a possible therapy of CLL. However, because of adverse reactions and excessive consumption of B lymphocytes, SYK inhibitor therapy has received a lot of skepticism.
Abstract
Over the last decade, targeted inhibition of Bruton's tyrosine kinase (BTK) has led to a paradigm shift in the way chronic lymphocytic leukemia (CLL) is managed. BTK inhibitors (BTKi) are broadly classified as covalent BTKI and noncovalent BTKi (cBTKi and ncBTK) Ibrutinib, as the first approved cBTKi, vastly improved outcomes for patients with CLL over prior chemoimmunotherapy regimens. However, long-term use is limited by both intolerance and resistance. The second generation of more selective BTKi were developed to improve tolerability. While these agents have led to an improved safety profile in comparison to Ibrutinib (both acalabrutinib and zanubrutinib), and improved efficacy (zanubrutinib), intolerance occasionally occurs, and resistance remains a challenge. The third generation of BTKi, which noncovalently or reversibly inhibits BTK, has shown promising results in early phase trials and are being evaluated in the phase 3 setting. These drugs could be an effective treatment option in patients with either resistance and intolerance to cBTKi. The most recent development in therapeutic agents targeting BTK is the development of BTK degraders. By removing BTK, as opposed to inhibiting it, these drugs could remain efficacious irrespective of BTK resistance mutations, however clinical data are limited at this time. This review summarizes the evolution and ongoing development of newer BTKi and BTK degraders in the management of CLL, with a focus of future directions in this field, including how emerging clinical data could inform therapeutic sequencing in CLL management.
''In conclusion, CAR19/22 T-cell therapy is efficacious in r/r aggressive B-NHL with TP53
alterations. Combining CAR-T cell administration with subsequent autologous stem cell transplantation (ASCT) further improves long-term outcome of these patients.''